Mahesh Shetty MD
In young, pregnant, breast feeding and the teenage women, the most common breast symptom is a breast lump. Other symptoms include a nipple discharge. Breast cancer is not common but important to be diagnosed early. Ultrasound of the breast is the initial tool to assess breast symptoms in these women.
Palpable breast lump
Palpable Breast lump is the most common reported breast symptom in pregnancy and lactation. Due to young age and the decreased accuracy of mammography because of dense breast tissue, breast ultrasound (US) is the first-line imaging examination in pregnant and lactating patients. If breast ultrasound is negative and does not explain the clinical findings, or if there are suspicious sonographic findings, additional imaging with mammography may be indicated. Diagnostic mammography is not contraindicated in pregnancy or during lactation.
Nipple Discharge during pregnancy
Nipple discharge in pregnancy may be physiologic, related to infection, trauma to the nipple, or caused by benign papillary tumors and uncommonly result from an underlying breast cancer. Spontaneous bloody discharge from the nipple is uncommon and usually manifests in the third trimester of pregnancy. Because of known association with pregnancy, appropriate evaluation including ultrasound is needed to exclude intraductal masses. Mammography is generally not helpful; spot magnification views of the retro areolar breast should nevertheless be performed to identify calcifications associated with the rare intraductal cancer. Cytology of the discharge is not helpful. Nipple discharge usually resolves in 2 months. Lobular proliferation, increased vascularization is the likely underlying factor and occurs in about 20% of pregnancy.
Pregnancy associated breast cancer (PABC)
PABC is breast cancer diagnosed during or within one year of pregnancy and reported to account for 4.3 % of all breast cancers and affects 1 in 3000 live births. The incidence is increasing as women defer childbearing age to the 4th and 5th decade. PABC tends to be diagnosed at a more advanced stage and with poorer prognosis compared to the non-pregnant patient. PABC is more likely to be triple negative and stage 3 and 4, with a 5-yr survival rate of 65%. Microenvironment changes induced in the breast tissue by pregnancy hormones may be contributory to aggressiveness of cancer in pregnancy. Delay in diagnosis is attributed to difficulty in clinical assessment of the breast due to pregnancy induced changes. A higher rate of inflammatory breast cancers has been reported, more than 50% present with lymph node involvement, nodal assessment is important once a suspicious finding is identified when evaluating a palpable lump.
- Most common clinical presentation is a painless palpable lump (86%), unilateral breast enlargement (6%), skin thickening, spontaneous bloody nipple discharge (8%), axillary lymph node enlargement or milk rejection are rarer presentation.
- Ultrasound has a 100% sensitivity in diagnosing PABC, most frequent finding is a mass. A solid mass with irregular margins was the most common finding on ultrasound.
Ultrasound shows a cancerous tumor in the breast in a pregnant patient who presented with an enlarging breast lump

Mastitis in Pregnancy
Painful swollen breast often with fever is the presenting symptom in infection of the breast. This infection is called mastitis is said to occur in 1-24% of breast-feeding women. Treatment is by antibiotics; ultrasound of the breast is performed mainly to identify a breast abscess. Breast abscess is reported to complicate puerperal mastitis in up to 44% of cases. The underlying factors are milk stasis, blocked ducts, or physical injury to the breast. Milk stasis provides a medium for bacterial proliferation. The bacteria causing the breast infection gains entry through cracked nipples during lactation originating from the nasopharynx or mouth of the infant and proliferate in the stagnant lactiferous ducts.
- Breast feeding is encouraged during mastitis to drain such engorged ducts.
- Breast feeding cessation is only advised following surgical drainage or if mother is on an antibiotic that is contraindicated for the newborn.
Ultrasound showing a breast abscess in a breast feeding woman with swollen painful breast and fever. The abscess was surgically drained.

Breast lump in a teen patient
Ultrasound is the only imaging modality that should be used in young women in their teens and twenties who have clinical problems. The indication is almost always for evaluation of a palpable mass. If the solid mass has the classic ultrasound appearance of a fibroadenoma, it will be followed for 24 months with ultrasound at 6- to 12-month intervals to confirm stability. Biopsy or excision is not indicated in the absence of unusual findings such as rapid growth, large size (greater than 5 cm), or other atypical ultrasound features.
Ultrasound shows a non-cancerous tumor in an 18 year old with a breast lump.

Breast Cancer in Young Women
Breast cancer is still the most common cancer in women younger than 35. There is evidence of increasing rate of breast cancer in the young population under age 40. The Group for Cancer Epidemiology and Registration in Latin Language countries (GRELL) study analyzing epidemiologic data from European countries showed the rate to be increasing by 1.2% every year from 1990-2008.Triple negative breast cancer, subtype with poorest outcomes, is more typically noted in premenopausal age group.
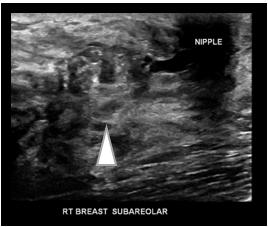
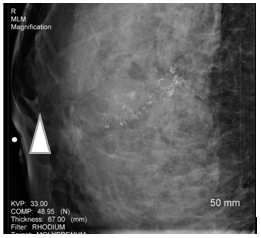
Ultrasound and mammogram in a 24 year old with a breast lump showing a cancerous tumor growing inside the duct (arrowhead)